If I Have a Blow Out in My Gastric Bypass Will I Have to Have Surgery Again
There are several things to consider when trying to determine between gastric bypass surgery and gastric sleeve surgery. Unlike the laparoscopic adaptable gastric ring (Lap Band), these two operations are both permanent, reduce hunger, and lead to the highest percentage of weight loss. To properly compare gastric sleeve surgery to gastric bypass surgery we will examine the following data :
- Expected weight loss.
- Speed of weight loss.
- Fourth dimension of surgery.
- Gastric featherbed benefits over sleeve.
- Gastric sleeve benefits over bypass.
- Risk of complications.
- Surgeon skill and preference.
Amount of Weight Loss
It'due south important to know how much weight you tin can expect to lose later surgery. It's every bit of import to know that long-term weight loss is more dependent on your lifestyle than which procedure you choose. Healthy do and eating habits will lead to more than weight loss than the averages beneath.
If you practise not implement salubrious lifestyle changes afterwards gastric bypass or gastric sleeve surgery, you lot can and probable will gain the weight back.
Gastric featherbed patients lose betwixt sixty to 80 pct of excess body weight in the first year. Gastric sleeve patients lose betwixt 50 to lxx percent of backlog body weight in ii years.
The Averages
For super obese individuals, a BMI over 45, gastric bypass is often recommended. Gastric bypass is preferred because information technology produces slightly more weight loss on average, and it creates 'dumping syndrome.'
Weight loss for average person.
Super obese patients frequently accept eating disorders and long standing love/hate relationships with nutrient. Because gastric bypass creates 'dumping syndrome' the patient is negatively reinforced with nausea, sweating, and a general 'ill' feeling before long after they eat sweets or big amounts of carbohydrates. This helps reduce binging and limits high-saccharide foods.
However, many surgeons are finding that gastric sleeve surgery is also very helpful with super obese patients.
Gastric sleeve surgery removes seventy% of the tummy where the hunger hormone ghrelin is produced.
This quickly and effectively reduces hunger and leads to excellent results in the super obese and other classes of obesity.
In fact, gastric sleeve surgery was originally created equally the first step in a multi-stage process for the super obese. Surgeons would create a sleeve and and so finish the rest of the procedure (re-route intestines) after the patient had lost some weight. However, most patients lost plenty weight from the starting time part of the procedure (the sleeve) that they didn't need a second procedure.
Use this figurer to find out how much y'all volition weigh later gastric sleeve surgery and gastric bypass surgery.
Regardless of which weight loss surgery you choose, you can look to lose a sure amount of weight from bariatric surgery. This reckoner will tell you how much weight you can wait to lose from each bariatric procedure and what you tin expect to counterbalance two years after surgery.
The calculations are based on boilerplate weight loss per procedure. To lose the average corporeality of weight, you'll need to follow your surgeon's pre-operative and post-operative guidelines.
Long term diet and exercise changes forth with other habit changes can pb to weight loss that exceeds the averages used in these calculations.
On boilerplate gastric featherbed patients lose about 70% (Bariatric Surgery, A Systemic Review and Meta Analysis, 2004) of their excess weight. Gastric sleeve patients lose nearly 60% of their backlog weight. And Lap Band patients lose about fifty% of their excess weight.
Comparison of Procedural Times
Going under anesthesia carries an inherent risk. The take a chance is college for people that are considered obese. It's even higher when you lot have co-morbidities similar high-cholesterol and high blood pressure. While a minor factor in your overall decision, process fourth dimension should be a factor in your determination.
By analyzing this information and calculation it to the other factors involved, an individual will be able to brand a more informed decision about which procedure might exist ameliorate suited for their needs.
In an article from Obesity Surgery entitled "A Review of Laparoscopic Sleeve Gastrectomy for Morbid Obesity," numerous studies were examined. The boilerplate procedural times for these two bariatric procedures were then calculated. The average length of time for the gastric bypass process was 2 hours and 44.8 minutes (164.8 minutes), and the average length of time for the gastric sleeve procedure was 1 hr and 40.iv minutes (100.iv minutes).
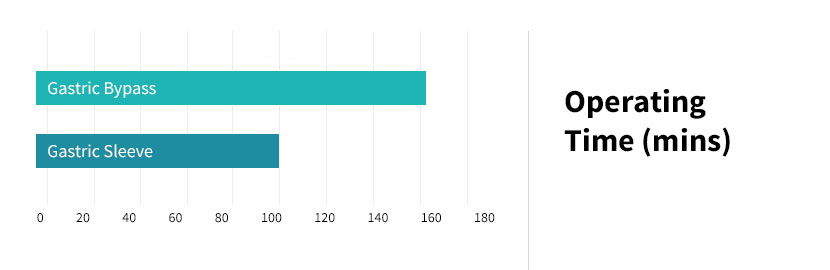
Chart showing operating times for gastric sleeve compared to gastric featherbed.
Comparison of Weight Loss Speeds
As mentioned at the kickoff of this article, weight loss is greater with gastric bypass surgery; even so, if given three years or more, the losses from gastric sleeve surgery brainstorm to catch up with the losses from gastric bypass surgery.
In addition, the Torso Mass Index (BMI) needs to exist factored into the equation considering this element of data will greatly affect the speed and amount of weight loss. The higher a patient's IBMI (Initial Torso Mass Alphabetize), the greater the driblet of the patient's BMI (especially after 3 years or more), regardless of procedure. Basically, the bigger yous are prior to surgery, the faster you'll lose weight.
WEIGHT LOSS SPEEDS
Gastric bypass produces almost all of its weight loss in the first year. Gastric sleeve surgery patients come across weight loss continue through year two before they hit their target weight.
Losing weight quicker will get you to a healthier weight faster where it becomes easier to exercise and go along to implement healthy habits. Notwithstanding, losing weight over a 2 year period may reduce saggy skin and stretch marks. Some patients prefer a gradual transition while others want to leave of their 'fatty arrange' as quickly as possible.
Unique Benefits of Each Procedure
Both procedures are extremely safe and while one procedure takes more than time (gastric bypass), this shouldn't be your 'aha' factor when choosing your process.
Gastric bypass surgery is considered the 'gold standard.' That sounds adept, right?
What'due south The Benefit of Gastric Featherbed Over Gastric Sleeve?
Many people will have different opinions on this question.
Why is gastric bypass considered the 'Gilt Standard' and gastric sleeve surgery non?
- Gastric bypass surgery has been around longer. Its results and complications accept been studied and its benefits proven. Every fellowship trained bariatric surgeon spent much of their preparation performing this procedure and the Lap Band procedure.
- Bypassing the intestines produces a malabsorptive aspect (less fourth dimension for your body to blot calories since your intestinal tract is shorter) that effectively reduces calorie consumption.
- Gastric featherbed is more complicated, has a slightly college overall take chances profile but information technology does produce more weight loss. And it creates dumping syndrome.
- If you have a history of acid reflux (GERD), your surgeon may recommend gastric bypass instead of gastric sleeve surgery. There is a lower run a risk of GERD after gastric bypass.
Dumping syndrome sounds like a complication and a horrible side-event of gastric bypass. It's not. It'southward a do good. And it'southward unique to gastric bypass surgery.
DUMPING SYNDROME
Also known as rapid gastric elimination, this condition occurs when too many sugary and/or fatty foods are consumed too speedily. The tummy and so dumps the food textile and gastric juices into the small intestine prematurely.
When an private undergoes gastric featherbed surgery, the pylorus is removed; this is the body's safety valve that prevents the contents of the stomach from elimination into the small intestine too quickly. The body reacts by releasing gastrointestinal hormones in the small intestine and secreting insulin. Non everyone gets or experiences dumping syndrome. However, reports show about fourscore% of gastric bypass patients will experience dumping syndrome.
Early Dumping
In that location are two types of dumping syndrome: early and late dumping. The symptoms for early dumping usually occur 15 to 30 minutes afterwards a meal and include nausea, diarrhea, cramps, bloating, dizziness, heart palpitations, sweating, and vomiting. You feel sick. Very sick.
Early dumping may occur if ane eats foods that are either as well cold or as well hot; it tin also be brought on by drinking liquids during a repast. The about common reason for early dumping is the consumption of sugary foods and large meals high in carbohydrates.
Late Dumping
Tardily dumping is a type of hypoglycemia (depression blood carbohydrate) and its symptoms unremarkably occur about i to three hours subsequently completing a meal. These symptoms include diarrhea, sweating, fatigue, weakness, dizziness, heart palpitations, fainting, and hunger. This condition may be controlled by consuming foods at a slower pace and by restricting one's intake of sugary substances. Generally, the condition is controllable; still, it tin become very serious if an individual continues to make poor dietary choices.
Why Dumping Syndrome is a Benefit
Remember Pavlov's dog? His dog would salivate every time he saw his food. Every bit he was testing how much the domestic dog would salivate, he noticed that the dog started to salivate every fourth dimension his researcher came into the room. The canis familiaris had begun to associate the researcher with his food and started to salivate when he saw the researcher.
Dumping syndrome is the Pavlov's dog experiment with a negative reinforcement. Once you experience your kickoff bout of dumping syndrome, your trunk is going to develop an farthermost dislike of sugary, carbohydrate filled foods. At minimum your mind will warn you not to consume that donut or that slice of block.
For people who have battled with obesity their entire life, this reminder and negative reinforcement helps curb consumption of unhealthy foods.
Other Possible Reasons Why Featherbed is the Gold Standard
Gastric Bypass is a circuitous operation performed by some of the most talented and highly trained laparoscopic surgeons. There is a level of pride in knowing how to perform this procedure. And non everyone tin can practise information technology. Information technology's the almost researched and studied weight loss surgery available. And it'south been around the longest and has thousands of success stories.
Benefits of Gastric Sleeve Over Gastric Bypass
Neither gastric featherbed nor the sleeve is reversible. Simply frankly, neither is the Lap Band (contrary to pop belief). Reversible implies it'southward easy to remove and while yous can remove the Lap Band, it requires a second procedure that is typically more difficult than the first. But that's another discussion.
Both procedures offer a similar weight loss profile, albeit you'll lose slightly more than with gastric bypass.
Gastric sleeve surgery does offer some benefits over gastric featherbed. The primary benefits are reduction of hunger and the speed and relative ease of the procedure. You will also require less vitamins after surgery.
The greater curvature (left side) of your stomach is idea to be the area where the hunger hormone ghrelin is produced. In gastric sleeve surgery this surface area is removed nigh entirely. The outcome is significantly reduced hunger. Some patients report having to remind themselves to eat for the first 6 months after surgery.
It's important to annotation that with gastric bypass yous do have a smaller pouch (stomach) and ghrelin production is besides reduced. However, there is some data that seems to indicate less hunger with gastric sleeve surgery post-operatively compared to gastric bypass.
- Another purported do good of gastric sleeve surgery is a slower weight loss profile. Typically, gastric sleeve patients run across their weight loss plateau afterward 2 years while gastric bypass produces much quicker weight loss (typically all inside the first year).
Why is information technology a do good to lose weight slower? This is very subjective and not proven. Some patients and medical professionals believe slower weight loss leads to less saggy pare and a reduction in stretch marks. It may likewise let you fool your co-workers into thinking yous've establish the greatest weight loss secret on earth, assuming you oasis't told them most your surgery.
Risk of Complications
The take chances associated with each process needs to exist looked at as well. This includes complications that might occur immediately afterwards surgery or several months later. Some of these complications are minor and some can be serious.
However, bloodshed (the risk of death) is not a major outcome with either surgery. This is especially truthful with laparoscopic cases. While open procedures accept a higher mortality charge per unit, it is withal below ane percent.
Complications of Gastric Bypass Surgery
For astringent complications call 911 emergency.
Complications can and practice happen.
Below is an overview of the common complications associated with gastric bypass. They are listed in order of least serious to nigh serious.
NAUSEA
Nausea is another common side effect of gastric bypass surgery. Post-obit the doctor's and/or nutritionist'southward recommendations for dietary intake usually improves this status. In addition, receiving a larger amount of IV fluids at a faster rate also assists with improving these complications. The average risk of nausea is 70%.
DEHYDRATION
Dehydration is a depletion of fluids and is very mutual later on gastric bypass surgery; nonetheless, information technology is usually managed if the patient drinks enough h2o in the weeks post-obit the surgical process. 2 liters a day is usually the corporeality of water that is recommended. Non consuming enough water may cause vomiting, which could lead to worse dehydration and other complications. If the aridity is severe enough, an individual may accept to receive more IV fluids. An individual'south run a risk for dehydration may be as high every bit 65% or more.
INDIGESTION
Dyspepsia (indigestion) can exist defined equally difficulty with digesting nutrient; this condition is accompanied with a burning awareness or discomfort in the upper abdomen. Treatment consists of changing ane'south diet past avoiding greasy foods. It may likewise exist treated by simply drinking liquids for a sure amount of time. Antacids and H2 blockers are used to treat this condition if dietary changes practice not work. A patient's take chances for indigestion is unremarkably somewhere around 60% or more.
REACTIVE HYPOGLYCEMIA
This situation occurs when a patient has low claret carbohydrate. Information technology generally occurs 45 to 60 minutes afterward eating a meal high in carbohydrates. Symptoms may include lightheadedness, increased centre rate, and sweatiness. This is considering in that location is an imbalance between claret sugar and insulin inside the bloodstream. Insulin allows saccharide to be processed, but if the insulin remains in the claret after the sugar from the repast has been used, then it causes low claret saccharide. Consuming a few ounces of diluted juice or 2 ounces of skim milk has proven to exist effective treatment for this condition. To prevent reactive hypoglycemia, an private should avert sugar and eat proteins first.
Equally a complication of gastric bypass surgery, hypoglycemia often occurs because of excessive dumping later on the surgery. Medications volition commonly manage conditions; still, surgical removal of a portion of the pancreas may exist required in more farthermost situations. The risk for this status is around ane percent.
NUTRITIONAL DEFICIENCIES
Thirty per centum of individuals who have gastric bypass surgery develop nutritional deficiencies. These deficiencies include osteoporosis, anemia, and metabolic bone illness. These deficiencies may be prevented with vitamin and mineral supplementation.
GALLSTONES
Individuals who take gastric bypass surgery have a 33% risk of developing this status. Gallstones are formed from pieces of cholesterol and other matter inside the gallbladder and/or bile passages. The possibility of getting gallstones increases dramatically when an individual experiences extreme weight loss. Prevention of gallstones may be achieved with bile salts. Some surgeons may remove the gallbladder during surgery in order to deal with this condition.
INCISIONAL HERNIA
This dangerous condition involves the intestine becoming obstructed. A hernia is an opening that occurs when an internal organ or trunk part protrudes through a surgical incision; it occurs inside the abdomen or through the abdominal wall muscles. An internal hernia may result from surgery and rearrangement of the bowel. An incisional hernia is an incision that does not heal in a right fashion. Intestinal wall hernia is more likely to occur with open procedures than with laparoscopic procedures and usually occurs several months after surgery. Although the charge per unit of this condition can be as high as 20% with open surgery patients, laparoscopic patients have a adventure of only 0.ii%.
WOUND INFECTION
Incisions may be infected considering of bacteria released from the bowel during the operation. This may as well happen to the inside of the belly; however, bladder and kidney infections may besides occur. Antibiotics, respiratory therapy, and physical activity afterwards surgery tin can lower these risks. These types of infections are far more common with open up surgery than with laparoscopic techniques. The average rate for developing this gamble is 12%.
MARGINAL ULCERS
Marginal ulcers are the most common in the newly created stomach pouch afterward gastric bypass surgery. They can usually be avoided past post-obit the correct dietary guidelines. They may besides exist avoided by not smoking and not using NSAIDs (including ibuprofen). These ulcers are oftentimes accompanied by a burning hurting in the tummy, and their presence can exist confirmed with an endoscopy (a scope inserted into the mouth and downwards the esophagus). They are ordinarily treated with antacids. Gastric bypass patients accept a 12% run a risk of developing ulcers.
STOMAL STENOSIS (STRICTURE)
A stricture is when a constriction of the opening to or from the tum becomes inflamed and/or blocked, preventing food from properly entering the stomach or intestines. Although this condition occurs with gastric sleeve surgery, it is most common in gastric bypass surgery and results from a build-upwards of scar tissue. Strictures tin be either acute or chronic (very quick onset or an ongoing issue after surgery). Symptoms include food intolerance, dysphagia, nausea, and vomiting. Strictures found immediately after surgery may be treated with bowel balance (non consuming food by oral cavity) and rehydration with intravenous fluids. These strictures will commonly heal, and if they practise non, and then endoscopic dilation is performed in order to restore the opening. The risk of this complication is 8%.
ANASTOMOTIC LEAKS
This condition occurs when a connexion made during surgery leaks digestive contents into the belly. This state of affairs may produce infections and can oftentimes exist stock-still if it is found rapidly plenty. By bravado air into the connection and using a dye, a surgeon can encounter if the connexion is secure. The risk for leaks is 5%.
HEMORRHAGE
Mutual symptoms of postoperative bleeding include hematemesis (vomiting of blood) or melena stools (bloody stools). There are ii types of hemorrhages: intraluminal and extraluminal. Intraluminal bleeding is often managed past using big bore intravenous lines for fluid resuscitation, administration of packed red blood cells, measurement of urine with a Foley catheter, and performing an urgent gastroscopy. Common sources for extraluminal bleeding include the gastric staple line, spleen, liver or intestinal wall. Urgent laparoscopy allows for the evacuation of the clot and control of the bleeding source. Hemorrhages tin also be treated by replenishing actual fluids, discontinuing the utilize of anticoagulation drugs, and past transfusion or performance. The run a risk of hemorrhage after gastric featherbed surgery is iii.ii%.
VENOUS THROMBOEMBOLISM
The coagulation of the blood is increased whenever the torso is injured or undergoes a surgical process. Sometimes, a clot in the veins of the leg will grade, break gratis, and so bladder to the lungs. This type of jell is called a pulmonary embolus, and it can be life threatening. It should also be realized that there is an increased possibility of this occurrence if the patient'southward body does non move much afterward the procedure. In order to combat this trouble, blood thinners are administered immediately before the surgical procedure is to begin. The risk of deep vein thrombosis or pulmonary embolism is around one percentage.
Complications of Gastric Sleeve Surgery
You'll notice the complications for gastric sleeve surgery are very similar to gastric bypass. For a thorough explanation of gastric sleeve complications, this commodity is recommended.
GASTROESOPHAGEAL REFLUX DISEASE
Gastroesophageal reflux affliction (GERD) is a long-term complication that is very common with gastric sleeve patients. It is characterized by periodic episodes of gastroesophageal reflux and usually accompanied by heartburn. Information technology often leads to histopathologic changes, which are microscopic structural changes in the esophagus. Information technology may besides lead to esophagitis, which is an inflammation of the esophagus.
It is usually treated with proton pump inhibitors. If symptoms persist, a gastroscopy (which is an exam of the esophagus, tum, and duodenum using an endoscope) is performed. The risk for GERD can be as high every bit 47%.
NUTRITIONAL DEFICIENCES
Like gastric featherbed surgery, complications relating to malnutrition are likewise possible. This is peculiarly true if the prescribed nutrient supplementations are non taken. The most common deficiencies occur with iron and/or calcium. While almost nutritional deficiencies are more mutual with gastric bypass surgery, there is an increased risk of folate deficiency with gastric sleeve surgery; therefore, folate levels of mail service-op gastric sleeve patients are often closely monitored. The risk for nutritional deficiencies subsequently gastric sleeve surgery is 12%.
STRICTURE (CHRONIC)
Chronic strictures mostly require endoscopic or surgical treatments. Treatment options depend on the length of narrowed portion. If the narrowing is short, endoscopic dilatation is used. Yet, if the narrowing is long and endoscopic dilation fails, so surgery is often necessary. Some patients have even required a gastric bypass in order to convalesce this condition.
GALLSTONES
Gallstones are also developed in individuals who have gastric sleeve surgery. This is because the overall take chances of getting them increases whenever anyone experiences an enormous amount of weight loss. In the aforementioned style every bit patients who have had gastric featherbed surgery, prevention of gallstones is usually achieved with bile salts. The chance for this complication can be every bit loftier as 23%.
STRICTURE (Acute)
This condition about ordinarily occurs with gastric featherbed surgery; however, it is sometimes seen in patients who have undergone gastric sleeve surgery. Similar strictures institute in gastric bypass patients, treatment is accomplished by not consuming food orally and by rehydration with Iv fluids. Endoscopic dilation is also performed occasionally on gastric sleeve patients with this condition. The risk for stricture (including chronic stricture) is three.5%.
VENOUS THROMBOEMBOLISM
Although the risk of this condition is much greater for gastric featherbed patients, it occurs to a lesser caste with gastric sleeve patients. The risk of deep vein thrombosis or pulmonary embolism with gastric sleeve patients is below one percent.
STAPLE LINE FAILURE
One of the more immediate concerns of gastric sleeve surgery, this attribute of the procedure is given special attention by surgeons, who spend a lot of extra time and effort in order to make sure that the newly created barrier performs correctly. When the staple line does fail, the patient will frequently experience an increase in heart rate. Other symptoms include breathing problems and/or an increment in body temperature. If the leak occurs a few days after surgery, laparoscopy may exist attempted in social club to find and repair the leak. However, if the leak begins a week or more than afterward the operation, then the area is drained and then either treated with stents or done out depending upon the stability of the patient. The overall risk for this condition (including delayed failure) is two.4%.
Other Considerations

Feel LEVEL OF YOUR SURGEON
The average learning curve of a surgeon is generally 100 surgeries or more. Because of this cistron, the experience of a surgeon should be carefully considered. In addition, many surgeons will have more experience with one process than the other, and this element should also be taken into consideration. This commodity discusses how to cull your surgeon.
Gastric Bypass is a complex operation performed past some of the most talented and highly trained laparoscopic surgeons. In that location is a level of pride in knowing how to perform this procedure. And not everyone can exercise it. Go along this in mind when asking for your surgeon'southward opinion on which procedure is right.
Ask him how many gastric featherbed procedures he has performed and how many sleeve procedures. Sympathize that gastric sleeve has merely go commonplace in the last v years and most insurance companies did not include coverage for this procedure until 2011.
PERSONAL OPINION OF YOUR SURGEON
An experienced surgeon should review your medical information as well as your lifestyle.
It oftentimes takes a third party to notice habits that y'all may non be aware you've created. Certain habits, like severe binge or emotional eating are difficult to stop. Gastric bypass may be more appropriate for you. Your surgeon has seen many patients and has records of their success and failures. Considering of these unique insights your surgeon'due south opinion should not be discounted
Have an open an honest discussion with your surgeon almost your fears and your goals. Y'all should walk away confident that you lot chose the best procedure for you.
Source: https://www.obesitycoverage.com/gastric-bypass-vs-gastric-sleeve-surgery/
0 Response to "If I Have a Blow Out in My Gastric Bypass Will I Have to Have Surgery Again"
Post a Comment